I began gender-affirming care in 2022. HRT brought me joy and a sense of autonomy. Top surgery followed in October 2024. But poor preparation, misgendering, and dehumanizing moments marked the process throughout.
Pre-op consultations included gatekeeping questions, required therapist letters, and body-shaming comments about my "womanly hips" while I was unclothed for photos. On surgery day, the surgeon marked incision sites, grabbed fat, and commented on "feminine" features. I joked about feeling like Michelangelo's David. The staff chuckled awkwardly, they couldn't relate to my choices about my own body.
A car accident one month post-op reopened my wounds. A staph infection followed. For over a year I felt completely detached from embodiment. Every follow-up visit triggered earlier violations.
What happened here is not unusual. Experiences like this are part of everyday life for many people. While the space itself was not the source of these challenges, it also did nothing to soften their impact.
Design cannot erase trauma, but it can choose not to make it worse.


I am a white, Latine, transmasculine person with direct experience as a patient in gender-affirming healthcare. I began HRT in 2022 and had top surgery in October 2024. My perspective shapes this project including its gaps. Personal experiences are clearly marked throughout, but they are not data. They are context.
Where my standpoint is limited particularly around race, disability, and immigration status I rely on researchers and community members with deeper lived and scholarly experience. Methodology is grounded in intersectional feminist and trans studies praxis.
ethics of care

Transgender people seeking gender-affirming outpatient care often arrive carrying histories of medical trauma, discrimination, and minority stress.
Clinic design can worsen these harms. Or it can support healing.
This project proposes a framework for an urban gender-affirming outpatient clinic serving HRT patients, surgery seekers, and all gender-diverse adults. It applies TiD's eleven domains across every design decision, treating each choice as a clinical act.
All adults across trans and nonbinary identities including those who use none of these terms. Intersectional dimensions are central, not supplementary. Race, class, disability, immigration status, and housing status each shape how a person moves through this building.
| HRT Patients | Surgery Seekers | |
|---|---|---|
| Core need | Trust, continuity | Privacy, control |
| Key vulnerability | Erasure over time | Gatekeeping trauma |
| Design priority | Relationship spaces | Empowerment in exam rooms |
Somatic Vigilance Across 5 Visits
Sharpe, C. (2016) · In the Wake: On Blackness and Being · Duke University Press · Ch. 4: The Weather
Anti-Blackness is not a storm. It is the weather, the total climate in which Black life is lived. It is not exceptional. It is the air.
The somatic vigilance diagram tracks a related condition: for Black and brown trans patients, the weather inside a clinic is never neutral. Each visit layers more data into a body already calibrated for threat. Design that ignores this does not eliminate the weather. It just refuses to name it.


Kimberlé Crenshaw's framework is not background context here. It is a design tool. Overlapping oppressions do not happen in sequence. The intake form, the waiting room, and the exam table can each activate compounded harm at the same moment. Domain 7 (Equity) demands we design for the patient most harmed not the average.
Race & Transphobia
Black and brown trans women face combined medical racism and anti-trans bias. Generic "inclusive" design is not enough.
Class & Access
Unhoused trans patients navigate survival stress before and during care. Space must not demand performance of stability.
Status & Safety
Undocumented patients face identity exposure risk at intake. Systems design is a safety issue, not an afterthought.
 Click to expand
Click to expand
This project is sited at an existing two-building medical office campus south of Seattle, currently available for lease. The building is already fully built out as healthcare space no conversion required. Design interventions proposed here are retrofits and programming decisions, not structural builds from scratch.
The site sits in Tukwila, a majority-minority city with one of the highest rates of linguistic and ethnic diversity in Washington State. It is accessible by transit and sits within the broader South King County region which has growing but underserved trans and gender-diverse populations.
Current campus tenants include HealthPoint, DSHS, Leidos QTC Health Services, and Olympic Heritage Behavioral Health next door.

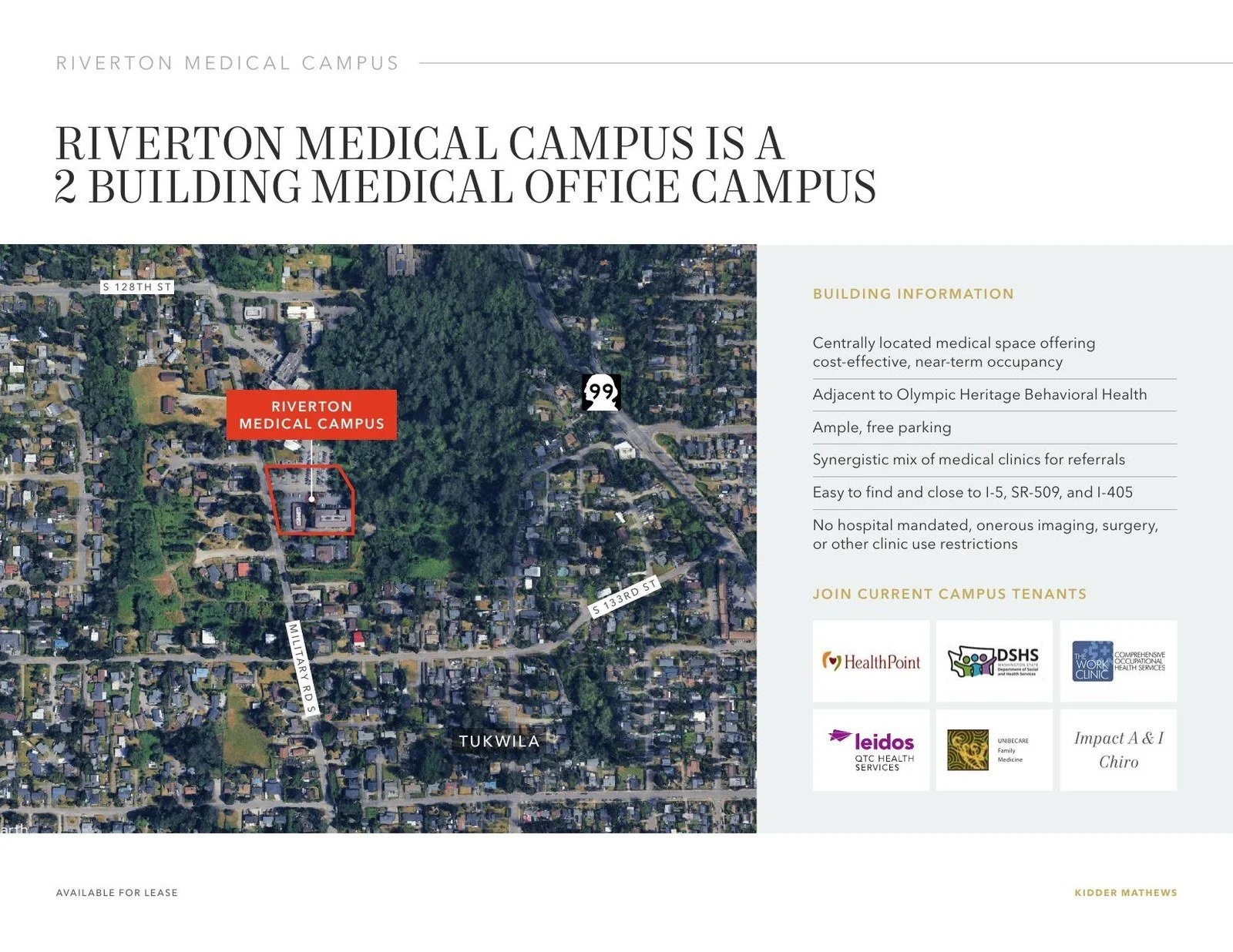
Riverton Medical Campus 13030 Military Rd S, Tukwila, WA. Adjacent to Olympic Heritage Behavioral Health. Current tenants: HealthPoint, DSHS, Leidos QTC Health Services.

Riverton Medical Campus in regional context Tukwila, WA. Adjacent to SeaTac Airport corridor, I-5, and South King County medical network: Kaiser Permanente, Virginia Mason Franciscan, Sea Mar, Valley Medical Center.
Site Advantage · Access
SeaTac International Airport is approximately 1.5 miles from this campus. For patients traveling in from out of state or out of country to see a private surgeon — a reality for many seeking gender-affirming surgical care — this proximity matters. The site is reachable by Link Light Rail with no car required.

13030 Military Rd S two-story, main campus entrance, monument signage visible from street

13050 Military Rd S single-story, landscaped entry, direct parking lot access
Both buildings show typical late-1970s medical office construction: stucco exterior, surface-level parking, minimal covered arrival, standard institutional signage. These are not obstacles they are the design brief.
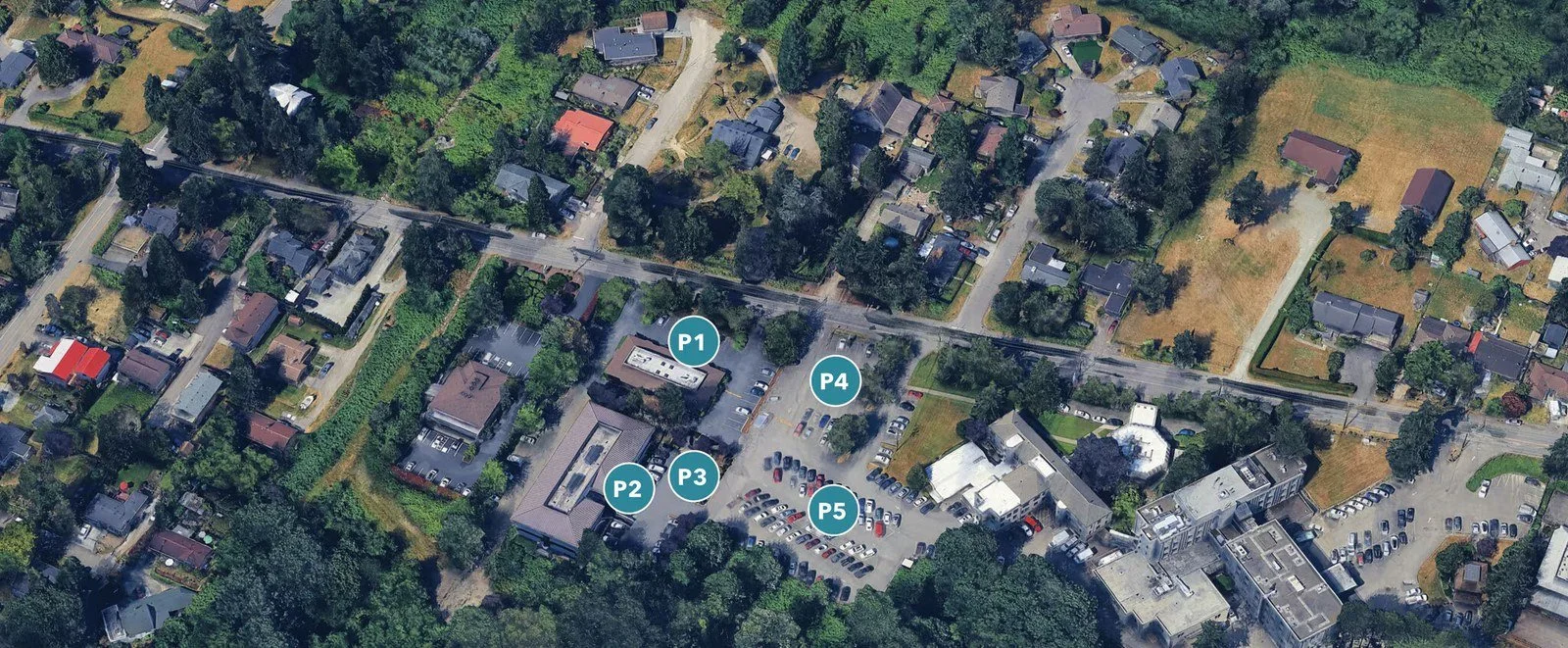
Campus parking lot open surface lot, no covered drop-off, monument signage legible from Military Rd S

Secondary view ample free parking, landscaping buffers, low-rise scale
The open parking lot is both an asset free, ample, accessible and a design problem. There is no covered transition from car to door. Patients arriving by transit or rideshare have no protection from public visibility at the moment of arrival.
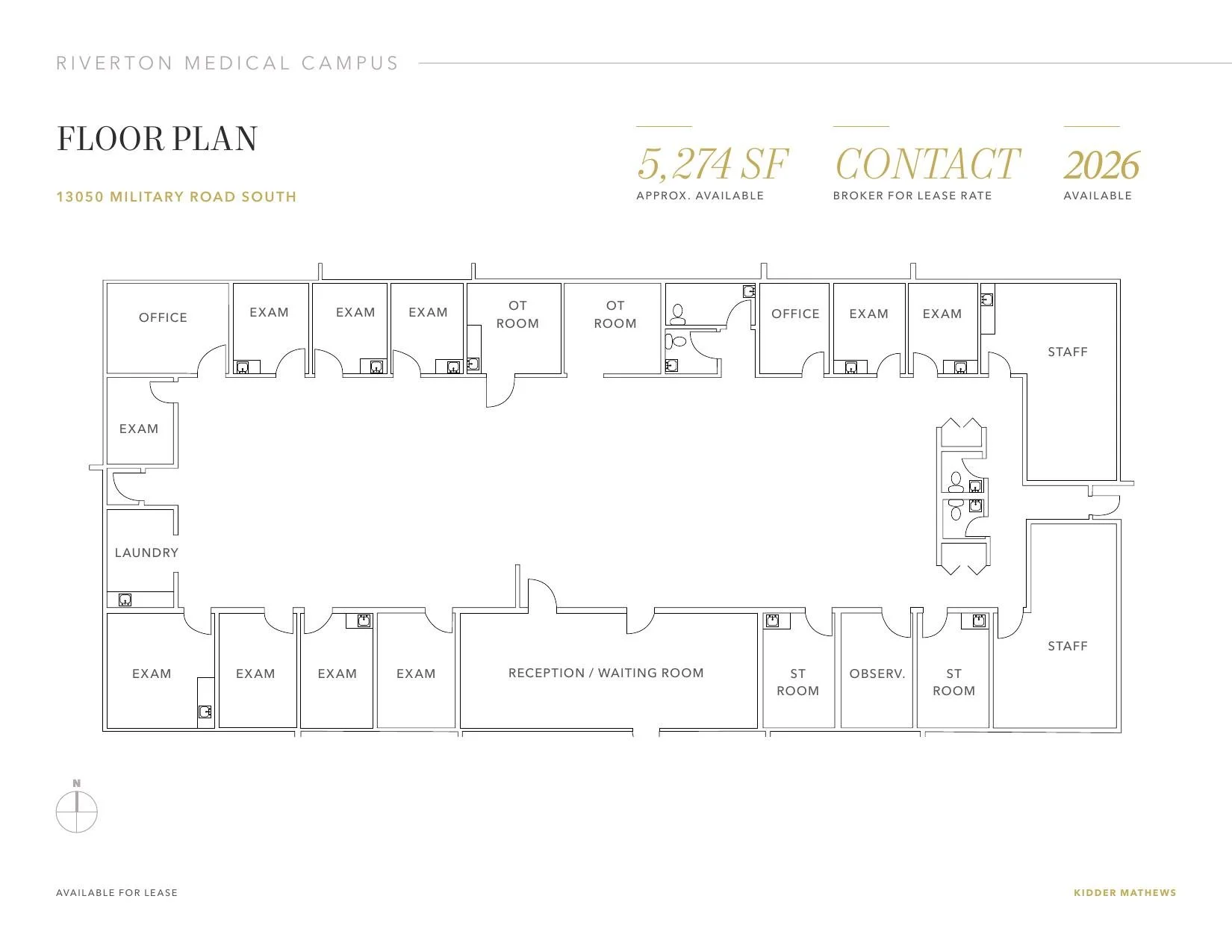
Building A 13050 Military Rd S · 5,274 SF · Single story · Existing healthcare build-out
- Open reception/waiting with no acoustic separation
- Binary bathrooms no all-gender facilities shown
- Exam rooms off a shared corridor sound transmission risk
- No patient-controlled lighting, gown options, or privacy signaling
- OT and observation rooms present but unspecialized
This is the starting point. The proposed Building A floor plan addresses each of these conditions through the lens of TiD's eleven domains.

Building B Level 1

Building B Level 2
- Two-story layout with elevator creates vertical patient circulation exposure
- Corridor-based exam room access, acoustic separation between suites unclear
- No dedicated surgical prep or recovery zones in existing build-out
- Binary bathrooms assumed, no all-gender facilities shown
- Level 2 specialty space lacks identifiable patient privacy protocol
Building B's two-story configuration is the more complex intervention: vertical circulation, dedicated surgery suites, and recovery spaces each require TiD thinking from threshold to discharge. The proposed Building B floor plan addresses each of these conditions in turn.
A single-story option (13050) eliminates elevator exposure entirely. Tenant-controlled HVAC gives the clinic direct control over thermal comfort. Ample free parking reduces transit exposure risk. No hospital-mandated use restrictions means the clinic sets its own intake protocols, gown policies, and signage from day one.
The multi-building campus creates the possibility of peer support and community programming in adjacent suites, a spatial expression of Domain 3 (Peer Support) and Domain 8 (Community).
Built in 1978, the building carries the assumptions of its era: binary bathrooms, open reception layouts, shared acoustic walls, institutional lighting. None of these are structural obstacles. All are design interventions this project directly addresses.
The goal is not a perfect building. The goal is a building made legible, safe, and affirming for people who have been harmed by spaces that looked just like this one.
Building A is the first building a patient enters. That is not incidental. It is the argument.
When I had top surgery, I met my surgeon for the first time in a consultation room that felt like every other clinic I had been in. Institutional, transactional, designed for efficiency rather than trust. By the time I was on the table, I had not had a single experience in that space that helped me feel safe.
Building A exists to change that. It is where you meet your doctor before anything clinical happens to your body. Where you ask questions, where you see your name used correctly on a form for the first time, where you sit in a waiting room that does not feel hostile. The single-story layout is not just a practical asset: it is a statement about what this first encounter should feel like. Accessible, unhurried, at human scale.
By the time a patient arrives at Building B for surgery, they have already been in this building. They know the campus. They know who they will see. That familiarity is not a luxury. For patients with histories of medical trauma, it is a clinical precondition for consent that is genuinely free.
Building A · 13050 Military Rd S
Single story, no elevator, existing healthcare build-out. Designated as the pre-surgery building: first contact, intake, consultations, HRT appointments, and all pre-operative visits. Patients meet their care team here before any clinical procedure. The single-story layout eliminates vertical circulation exposure entirely.
Building B Level 1 · 13030 Military Rd S
Dedicated surgery floor. Surgical suites, prep rooms, scrub zones, recovery bays, and staff support spaces. Patients arrive here on surgery day only, following a known pathway established during Building A consultations. Privacy checkpoint controls entry from the shared campus.
Building B Level 2 · 13030 Military Rd S
Specialty and post-operative services: endocrinology, gender-affirming specialty care, post-op follow-up, and wraparound support. Reached via elevator or stair from Level 1. Separating this floor from active surgery keeps post-op patients out of surgical circulation and creates a calmer recovery-oriented environment.
Patient Journey · Building Assignment Rationale
Building A exterior, 13030 Military Rd S
Click to expand
Campus surface parking, no covered approach
The problem: the parking lot is the first moment of exposure. For trans patients, particularly those who are visibly gender-nonconforming or BIPOC, an unstructured, unsecured arrival space with no affirming presence is itself a barrier to care.
Queer-affirming exterior security presence, STR8 UP Security, Seattle
D1 Safety + D7 Equity, security personnel who share lived experience with the patient population remove a documented point of harm. A uniformed queer guard is not just safer; it is a visible signal that this space was designed for you.
S1 Policy: met through a vendor procurement policy that prioritizes LGBTQ+‑owned and OMWBE‑certified contractors, this is a clinic operations decision, not just a design one. · S3 Built: met through the physical transformation of the exterior arrival sequence, a queer presence in the parking lot changes the spatial experience of approach.

str8upseattle.com
"Redefining security professionalism through industry-leading integrity, accountability, and customer-first standards."
Covered canopy walkway from parking to building entry, all-weather approach
D10 Movement + D1 Safety: continuous covered arrival eliminates the moment of unprotected outdoor exposure between car and door. For a patient who is visibly gender-nonconforming, a 30-second walk across an open lot is not trivial. The canopy is a mobility intervention as much as a comfort one.
S3 Built: met through construction of a post-and-trellis canopy structure spanning from the accessible parking zone to the building entry, a capital improvement item within the scope of a tenant improvement allowance.
Planting buffers along lot perimeter, ornamental grasses and low trees screen street view
D1 Safety + D9 Comfort: dense perimeter planting reduces visual exposure from Military Rd S, a patient arriving by car or rideshare is no longer visible from the street. Soft landscaping also signals this is not a generic commercial parking lot.
S3 Built: met through landscape design and site work, species selection, planting density, and bed placement are built environment decisions within the tenant improvement scope.
Defined lot perimeter with low fence or bollard line and a staffed guard booth at entry
D1 Safety + D2 Trustworthiness + D5 Empowerment: an enclosed, defined lot communicates intentionality. The guard booth staffed by affirming personnel (see STR8 UP Security) creates a clear, controlled arrival environment. Patients know where the lot ends and who is present. Ambiguity is a threat signal; definition is safety.
S1 Policy: staffing the guard booth, setting hours, and establishing protocols for who enters the lot are clinic operations decisions that must be embedded in security policy. · S3 Built: met through site design, bollard installation, fence or hedge boundary, and guard booth construction are capital improvements within the tenant build-out.

Campus perspective Riverton Medical Campus. Covered canopy connecting parking to entry, side drop-off zone with curb cut, low-profile signage. Building A: Intake, Welcome & Consultations. Building B: Dedicated Surgery Space.

Site plan, drop-off zone between buildings, new curb cut, covered path to entry. Building A: Intake, Welcome & Consultations. Building B: Dedicated Surgery Space.
- Monument signage visible from Military Rd S
- Surface parking with no covered approach or drop-off zone
- Building exterior reads as generic medical office
- No wayfinding that signals affirming intent
The problem: visibility from the street forces patients to choose between being found and being seen. For a trans patient, especially one who is Black, brown, or visibly gender-nonconforming, those are not the same thing.

Post & trellis entry canopy with exposed wood beams
D1 Safety + D9 Comfort eliminates the moment of public exposure before care begins; warm material language signals this is not a standard institutional space.
S3 Built: met through architectural addition of a covered canopy structure at the entry, a physical design intervention that transforms the threshold experience.
Discreet affirmative signage clinic name only, inclusion-focused language
D2 Trustworthiness + D7 Equity no identity disclosure from the street; legibility without exposure, especially for patients navigating unsafe home environments.
S1 Policy: the clinic name, branding, and public-facing language are institutional policy decisions, what the clinic is called and how it presents to the street is set at the administrative level. · S3 Built: met through physical signage design, scale, placement, and material choices that make the building legible without outing the patient.
Side drop-off zone with new curb cut & designated stalls
D10 Movement + D1 Safety transit and rideshare arrivals move directly to entry without crossing exposed parking; removes the most vulnerable moment in the approach sequence.
S3 Built: met through site engineering, new curb cut, paved drop-off zone, and stall designation directly alter the physical approach sequence.
Enhanced landscaping with native plantings & paver forecourt
D9 Comfort + D7 Equity sensory welcome that reduces hypervigilance before entering; fragrant lavender and native shrubs are also a cultural signal that this space was designed with intention.
S3 Built: met through landscape design, plant selection, paving material, and spatial layout of the forecourt are built environment interventions.
Remove any security desk or uniformed presence from entry sequence
D1 Safety uniformed security is a documented trauma trigger for trans people of color navigating policed urban space. Its absence is itself a design decision.
S1 Policy: the decision not to employ uniformed security at entry is an institutional policy, it must be explicitly written into clinic operations and staffing guidelines. · S3 Built: met through spatial planning, no desk footprint, no visual cue of surveillance at the threshold.

Final proposed floor plan, Building A, 13050 Military Rd S. Spatial layout incorporating TiD programming decisions.
- Open reception/waiting no acoustic separation
- Standard counter-height desk configuration
- Binary intake forms no chosen name or pronoun fields
- Shared corridor between check-in and exam rooms
The problem: open reception desks make every interaction semi-public. Names, insurance, pronouns audible to anyone in the room. For undocumented patients and those in unsafe home situations, this is not just discomfort. It is risk.
Lowered, angled reception desk private eye-level conversation zone
D2 Trustworthiness + D6 Choice replaces the counter transaction with a human interaction; patients choose how much to disclose and to whom.
S3 Built: met through custom millwork and furniture specification, desk height, angle, and screen positioning are built environment decisions.
Partial acoustic partition between check-in and waiting
D1 Safety + D9 Comfort contains clinical conversation; no one in the waiting room can overhear intake information.
S3 Built: met through architectural partition, a fixed or demountable element that physically separates the acoustic zones of reception and waiting.
Redesigned intake forms chosen name, pronouns, open gender identity field, name-use confirmation
D2 Trustworthiness + D7 Equity the first form a patient completes signals whether they are seen; binary forms erase nonbinary identities before care even begins.
S1 Policy: forms are an administrative policy instrument, their content, field structure, and data handling are set at the institutional level and must be approved and maintained as policy. · S2 Process: informed by lived experience of what patients wished they had been asked, this design process finding directly shaped the field choices.
Self-check kiosk option for patients who prefer minimal verbal interaction
D5 Empowerment + D6 Choice removes the mandatory social performance of check-in; patients direct their own arrival experience.
S1 Policy: the kiosk must be supported by an opt-in protocol, patients need to know it exists, and staff must be trained not to redirect kiosk users to the desk. · S3 Built: met through technology procurement and spatial placement, the kiosk is a physical object in the room with specific siting requirements.
Anonymous patient and staff feedback channel, physical card box plus digital QR option
D5 Empowerment + D2 Trustworthiness: patients and staff who experience harm or see a gap should have a clear, low-barrier, anonymous way to say so. A card drop box in the waiting area and a QR-linked digital form make feedback structurally available rather than dependent on individual willingness to escalate. This applies to both the patient experience and the staff experience of working in this clinic.
S1 Policy: a feedback mechanism is inert without a policy that mandates who reads submissions, how frequently, what happens when a pattern emerges, and how responses are communicated back. The box is a built environment element; the loop it closes is entirely a policy instrument. · S2 Process: ongoing patient and staff feedback is itself a design process tool that should inform future iterations of the clinic's spatial and operational programming. · S3 Built: met through placement of a physical card box and QR code display in the waiting area, visible and accessible to all patients and staff.

Building A Learning Center. Warm wood ceiling, abundant planting, flexible seating. Pronoun education whiteboard visible.
The Learning Center supports ongoing staff education and certification, including trans cultural competency, pronoun and identity affirmation, trauma-informed care practice, and clinical updates. It is not a break room. It is infrastructure for care quality.
Dedicated training space with flexible seating and display surfaces
D4 Collaboration + D8 Community staff who learn together are better equipped to maintain a consistent, affirming standard of care across every patient interaction.
S1 Policy: allocating a dedicated room to staff education is an institutional policy decision, space could instead be used as a break room or storage; designating it for learning is a governance choice. · S3 Built: met through room programming and interior fit-out, flexible furniture, writable surfaces, and AV infrastructure are built environment decisions.
Trans experience curriculum: identity, language, gatekeeping history, and lived harm
D2 Trustworthiness + D3 Peer Support clinical staff who understand trans experience are less likely to cause incidental harm; training is a structural commitment, not a one-time event.
S1 Policy: curriculum content, delivery schedule, and mandatory participation are institutional policy requirements, they must be embedded in employment contracts and onboarding, not offered as optional professional development. · S2 Process: the curriculum content was shaped by the design process, lived experience of care failures (misgendering, gatekeeping, body-shaming) directly determined what staff need to understand.
Ongoing certification pathways displayed and tracked by staff
D4 Collaboration accountability structures for continued education signal institutional commitment, not just individual goodwill, to affirming care standards.
S1 Policy: certification requirements, renewal timelines, and consequences for non-completion are entirely policy instruments, tracking and display make a policy commitment visible in space, but the commitment itself must exist in clinic governance first.

Staff Rest & Green Space, Building A. Indoor water feature, full-height glazing, tropical planting, soft seating clusters for peer debrief.
Staff who provide gender-affirming care carry significant vicarious trauma load, particularly in the current political climate. A space explicitly designed for staff recovery is not a perk. It is a clinical infrastructure decision.
Domain 11 (Play) is not about entertainment. It is about restoration, the conditions under which people can return to difficult work without burning out or causing harm.
Indoor water feature, full-height glazing, tropical planting
D9 Comfort + D11 Play: biophilic design is evidence-based for stress recovery; the space signals that staff restoration is taken seriously as a clinical investment.
S3 Built: met through interior design and construction, water feature installation, glazing specification, and planting are built environment elements that physically change the sensory quality of the space.
Soft seating clusters, small round tables, informal peer debrief space
D4 Collaboration + D8 Community: staff can process difficult interactions in a space designed for it. The layout makes peer support the default, not the exception.
S1 Policy: protected time to use this space requires institutional policy, without it, the furniture goes unused. · S3 Built: seating cluster configuration directly shapes whether peer debrief happens organically.
No clinical equipment, no patient-facing materials, staff space only
D6 Choice + D9 Comfort: staff choose when to enter; the space makes no demands. The absence of clinical cues is itself a restorative design decision.
S1 Policy: staff-only designation requires institutional policy or the space will be repurposed for storage or overflow. · S3 Built: the absence of clinical equipment is a programming decision about what is and is not installed.
- Open plan standard row seating configuration
- Generic healthcare imagery assumed throughout
- No acoustic treatment or sub-zone differentiation
- Single large shared space with no privacy options
The problem: open rows of seating leave patients exposed and visible to one another. Being visibly gender-nonconforming in an unstructured waiting room is a documented driver of healthcare avoidance; patients leave before being seen.

Proposed waiting room rendering. Art by Mister Samo, trans artist and activist.
Semi-private seating bays low shelving and planting as soft dividers
D1 Safety + D9 Comfort reduces exposure without isolation; patients choose their level of visibility within the space.
S3 Built: met through furniture layout, low millwork partitions, and planting, spatial sub-zoning is a built environment tool.
Trans-affirming community art local trans artists commissioned where possible
D7 Equity + D8 Community representation on walls is a clinical signal; patients see themselves reflected before a provider enters the room.
S1 Policy: an arts procurement policy that prioritizes local trans artists is an institutional equity commitment, it must be embedded in the clinic's purchasing and commissioning guidelines. · S2 Process: participatory selection of artwork, involving trans community members in choosing what is displayed, is a design process method that grounds representation in actual community voice. · S3 Built: met through the physical installation of artwork in the waiting room, scale, lighting, and placement are spatial design decisions.
Peer support wall community organizations, legal aid, housing, trans-competent providers
D3 Peer Support + D8 Community the clinic is not the only source of care; connecting patients to the broader ecosystem is part of the clinical act.
S1 Policy: maintaining and vetting the organizations displayed on the peer support wall is an ongoing policy responsibility, who is listed, how referrals are made, and how the wall is kept current must be written into clinic operations. · S3 Built: met through physical wall design, the display surface, mounting, and spatial integration of the peer support feature into the waiting room.
Acoustic ceiling panels reduce ambient noise, contain conversation
D9 Comfort + D1 Safety sound containment protects disclosures made in the waiting room; patients overhearing clinical conversations is a documented anxiety driver.
S3 Built: met through specification of acoustic ceiling tile systems, an architectural material and construction decision.
Patients undergoing gender-affirming surgery frequently report receiving inadequate pre- and post-operative guidance. Paperwork is dense, instructions are generic, and peer knowledge, the practical wisdom of people who have been through the same procedure, is rarely built into the clinical experience.
The problem: institutional care packets are written for a generic patient. They do not account for the specific recovery realities of gender-affirming procedures, and they are almost never written by or with trans people who have navigated them.
After my own top surgery, I did not receive much in the way of preparation materials. The practical knowledge I relied on came from other trans people online: keep a cup with a straw so you don't have to tilt your head back, use a grabber so you don't lift your arms, sleep at an incline, keep your drains labeled. None of this was in any packet. A clinic that takes TiD seriously would make peer knowledge a clinical input, not an afterthought.

Trans-authored pre-op and post-op care packets, co-written with people who have had the procedure
D3 Peer Support + D5 Empowerment: care packets written by trans people who have been through the same surgery carry different information than clinically authored materials. Practical tips, emotional preparation, what no one told you. This is peer knowledge formalized as clinical resource.
S1 Policy: the clinic must commit to co-authoring, maintaining, and distributing trans-authored materials as part of its standard care package, not as a supplement. · S2 Process: participatory authorship, involving patients with lived surgical experience as content contributors, is a design process method.
Dedicated pre-op appointment for questions only, no examination, no clinical procedure
D4 Collaboration + D2 Trustworthiness: a standalone appointment for the patient to ask questions without a clinical agenda changes the dynamic entirely. The provider is in listening mode. The patient has prepared. Nothing is happening to their body. This is collaborative preparation, not intake processing.
S1 Policy: scheduling a question-only pre-op appointment as standard practice requires institutional commitment; it takes provider time and must be protected from being folded into other appointments.
Recovery resource display: curated peer tips, practical supplies checklist, community referrals, stocked in waiting room and pre-op suite
D8 Community + D6 Choice: practical peer knowledge displayed as a clinical resource, cup with a straw, a grabber, sleeping inclined, drain care, not buried in a generic packet but visible, accessible, and authored by people who have been through it. Patients take what is useful to them.
S1 Policy: maintaining and updating this resource display is an ongoing clinical responsibility, not a one-time task. · S3 Built: met through a dedicated display surface in the waiting room and pre-op suite, spatial placement makes peer knowledge a visible part of the care environment.
Optional peer buddy match: patients connected with a trans person who had the same procedure, pre- or post-surgery
D3 Peer Support + D8 Community: one person who has been through the same surgery and can answer the questions you are too embarrassed to ask your surgeon. This is the most common form of trans healthcare knowledge-sharing. The clinic formalizing it treats that knowledge as what it is: clinical infrastructure.
S1 Policy: a peer buddy program requires opt-in consent, privacy protocols, vetting of participants, and staff coordination. It must be designed with the same rigor as any other clinical support program. · S2 Process: the matching process, who is matched with whom and how, is a participatory design decision that should involve trans community input.

All-gender single-stall restroom, Building A. Warm wood vanity, adjustable swivel mirror, grab bars, community art wall, menstrual products stocked without gender labeling. Warm ambient lighting, no overhead fluorescent.
- 1978 construction binary-gendered multi-stall bathrooms assumed
- No all-gender facilities noted in existing plan
- Standard institutional fixtures and overhead lighting
59% of 2015 U.S. Transgender Survey respondents avoided public restrooms due to fear of confrontation. The bathroom is not a peripheral concern, it is often the decisive one.
All-gender single-stall restrooms, floor-to-ceiling partitions, full-height door hardware
D1 Safety + D7 Equity: the minimum standard for this facility type; multi-stall gendered bathrooms are not acceptable in a gender-affirming clinical setting.
S1 Policy: designating all restrooms as all-gender requires updating facility signage policy, lease agreements, and staff training on how to direct patients. · S3 Built: met through renovation, floor-to-ceiling partitions and full-height door hardware are construction interventions that achieve physical privacy.
Occupancy-based signage: "In Use / Available", no gender symbols
D2 Trustworthiness + D6 Choice: removes the act of gender self-identification from bathroom access entirely.
S1 Policy: eliminating gendered signage is an institutional policy choice that must be adopted building-wide and maintained against facilities pressure. · S3 Built: met through specification and installation of occupancy indicator hardware on each door.
Warm recessed lighting + adjustable swivel mirror + hooks at multiple heights
D5 Empowerment + D9 Comfort + D6 Choice: warm lighting eliminates harsh overhead exposure; the swivel mirror gives patients control over what they see and when; hooks at multiple heights serve all bodies and mobility needs.
S3 Built: met through fixture specification and installation, lighting type, mirror mounting hardware, and hook placement are interior design decisions that require no structural change.
Health materials and menstrual products stocked without gender labeling
D7 Equity + D8 Community: removes the moment of gender-based gatekeeping from basic health supplies; supplies are openly stocked in wicker basket presentation, normalizing access without surveillance.
S1 Policy: what is stocked, how it is labeled, and who is responsible for restocking are supply chain and procurement policy decisions, the dispenser in the room is inert without an ongoing operational commitment behind it.
Grab bars + integrated bench seating, rose-gold hardware, dignified not clinical
D5 Empowerment + D9 Comfort: accessible design that does not signal disability, rose-gold finish and warm material integration make grab bars and bench seating feel intentional rather than institutional.
S3 Built: met through fixture specification, hardware finish, bench depth, and mounting height are spatial design decisions that determine whether an accessible feature feels dignified or clinical.
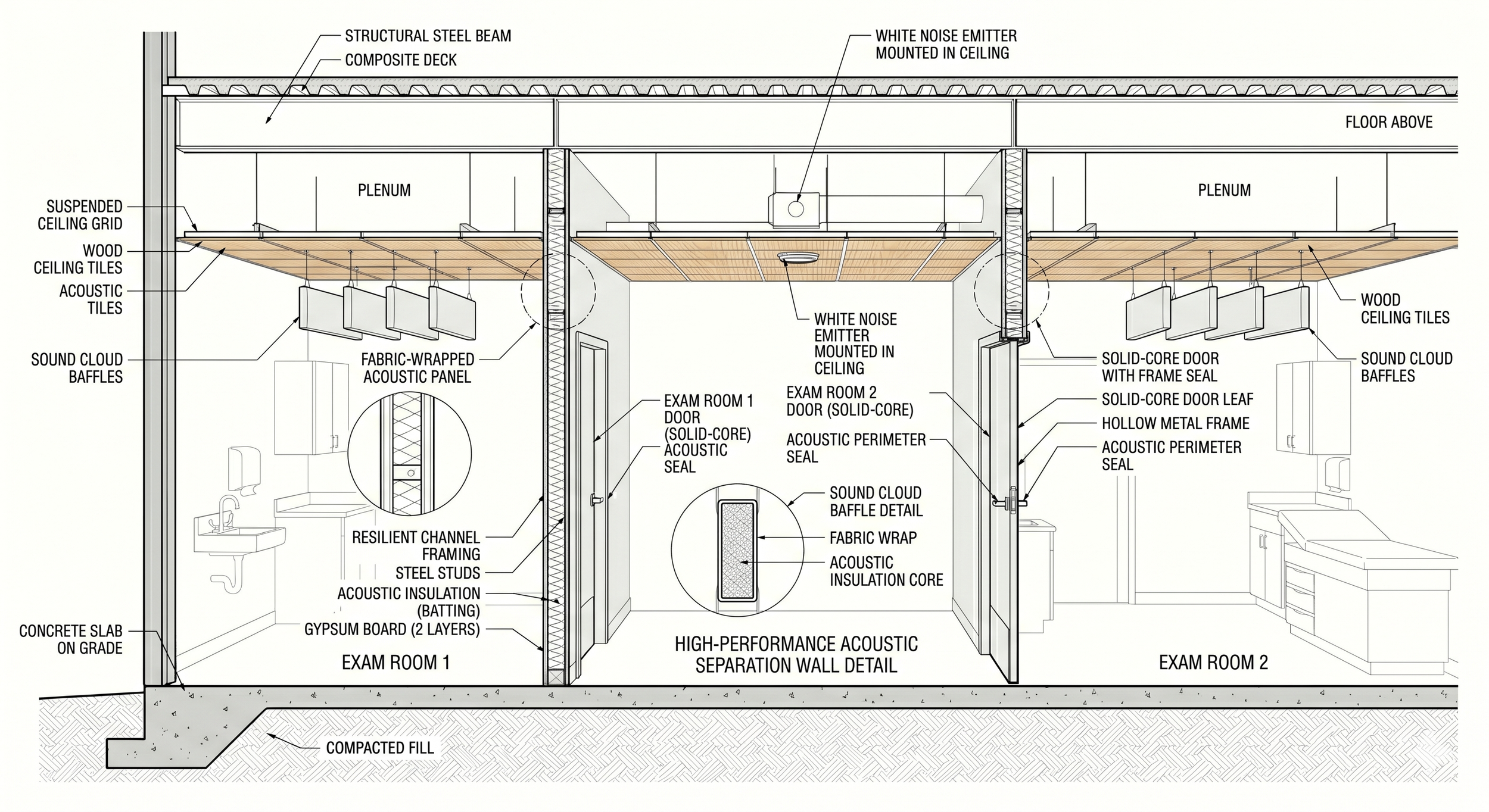
Longitudinal building section, Exam Room cluster, Building A. Resilient channel framing, solid-core doors with acoustic perimeter seals, wood ceiling tiles on suspended grid, suspended sound cloud baffles, and ceiling-mounted white noise emitters.
Post-op, I could hear everything from the neighboring bay. I heard a nurse misgender someone else. I spent the next hour waiting for it to happen to me.
The problem: a building where patients can hear each other is a building where no one feels safe disclosing. Acoustic privacy is a clinical need, not a luxury.
White noise emitters in corridor and reception zone
D1 Safety + D9 Comfort: masks clinical conversation without altering spatial layout; low-cost, high-impact. Ceiling-mounted emitters add broadband masking signal, clinical conversation is unintelligible to adjacent spaces.
S3 Built: met through technology installation, emitter placement, volume calibration, and zone coverage are built environment specifications.
Frosted film on glass-panel walls between provider workspaces and patient circulation
D2 Trustworthiness + D1 Safety: EHR data and provider workstation screens are not visible from patient areas.
S3 Built: met through material application, window film is a low-cost built environment modification that changes the visual permeability of existing glazing.
Resilient channel framing + acoustic insulation batting in exam room walls
D9 Comfort + D6 Choice: steel studs + resilient channel + insulation batting + two layers gypsum board. Mechanically decouples wall surface from structure, patients can speak at normal volume without monitoring themselves.
S3 Built: met through construction, resilient channel framing is a structural modification to the wall assembly that physically reduces sound transmission between rooms.
Solid-core doors + acoustic perimeter seals to all exam rooms
D1 Safety + D2 Trustworthiness: hollow-core doors transmit conversation clearly, solid-core door leaf in hollow metal frame with full acoustic perimeter seal is a structural baseline, not an upgrade.
S3 Built: met through door specification and replacement, solid-core doors with proper frame seals are a straightforward construction upgrade with direct acoustic impact.
Surgery day arrival at Riverton Medical Campus. The covered canopy, drop-off zone, and low-profile signage serve a heightened purpose on surgery day: patients are often accompanied, post-operative, or managing physical and emotional vulnerability. The same TiD interventions applied to Building A's intake approach carry through here to Building B. Building A: Intake & Consultations. Building B: Surgery Suite.
Site plan, surgery day patient flow. The drop-off zone is positioned between buildings to minimize the distance from vehicle to Building B entry; the covered path eliminates outdoor exposure after surgery. Patients returning to Building A for post-op consultations use the same covered link. D10 Movement is met through the site plan itself, sequencing matters as much as space.

Sage green and warm cream exterior palette
Replaces institutional dark teal with a calm, residential-scale material language.
The body reads a building before entering it. An institutional palette activates vigilance. A warm, residential palette lowers the threat register: clinical safety, communicated through material.
S3 Built Environment
Cedar-slat covered entry canopy
A protected threshold between parking lot and door. Patients are not exposed crossing open asphalt.
The canopy creates a liminal space where the body can regulate before entering. Wood underside reads as warmth rather than infrastructure.
S3 Built Environment
Native PNW hedge & fern privacy screen
Sword ferns, dogwood, ornamental grasses buffer the walk from car to entry.
Privacy in the arrival sequence is a safety issue, not an amenity. A planted buffer reduces the visibility of patients moving from vehicle to door.
S3 Built Environment
Human-scale bollard lighting
Warm 2700K bollards at human height illuminate the path without surveilling the person.
The shift from overhead floodlight to pathway bollard is a shift from institutional oversight to human welcome.
S3 Built Environment
Address-only ground sign: 13030
No clinic name, no medical branding visible from the street.
Discretion is a clinical safety feature. The S1 decision to suppress public branding is made legible through the S3 sign specification.
S1 Policy & Practice, S3 Built Environment
Designated drop-off zone with warm paving
A dignified arrival point with curb cut and bollard definition.
Choice at arrival is empowerment. A drop-off zone acknowledges that not every patient drives alone or can walk from a distant stall.
S3 Built Environment
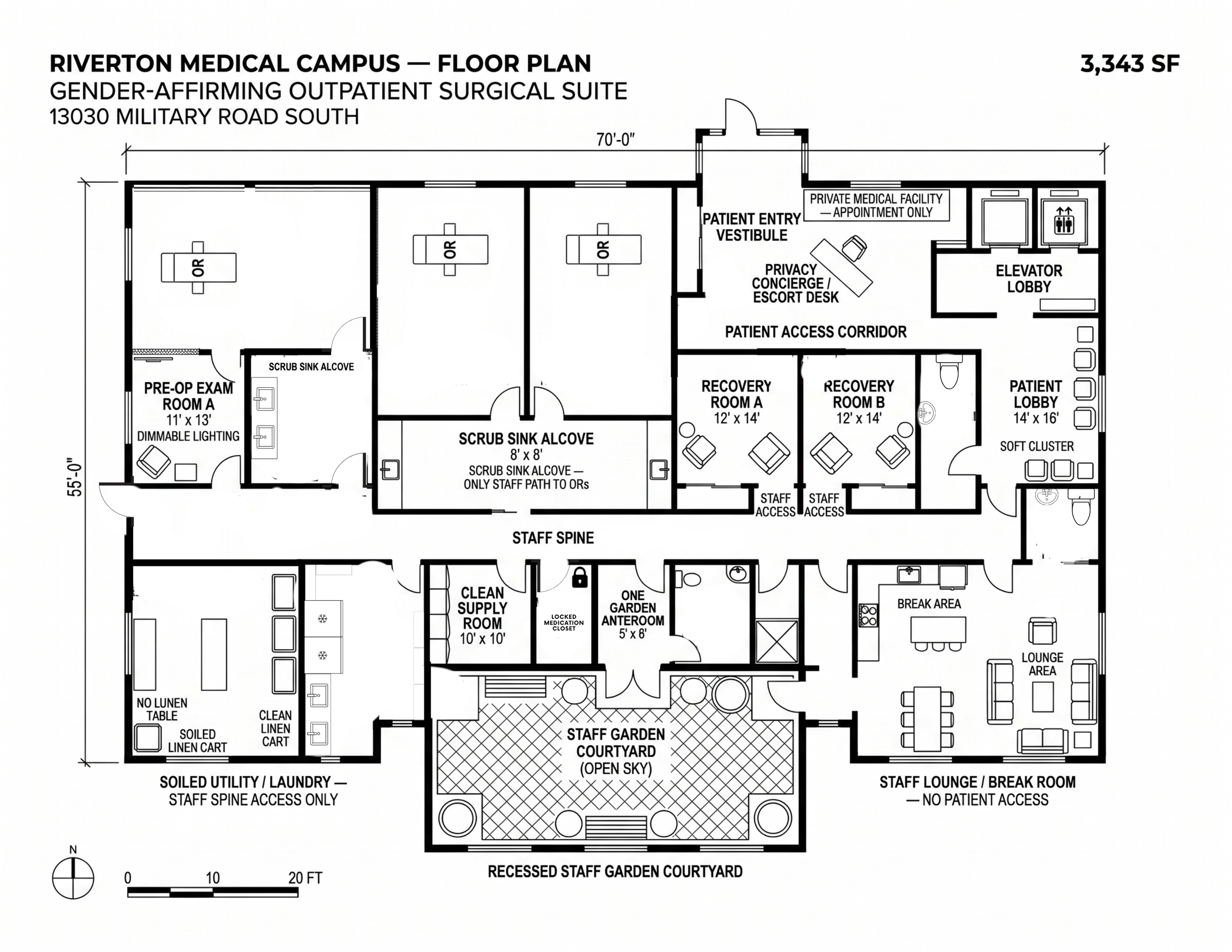
Proposed floor plan, Building B, 13030 Military Rd S. Level 1: surgical suites, prep, recovery, staff spaces. Level 2: specialty care and post-operative services.
Privacy checkpoint at elevator lobby
Controlled entry to Level 1 surgery floor
D1 Safety + D2 Trustworthiness: patients access the surgery floor through a staffed privacy checkpoint, not an open lobby. Only confirmed surgery-day patients and their companions enter. The spatial sequence communicates institutional protection before clinical contact.
S1 Policy + S3 Built
Two surgical suites with independent prep rooms
D6 Choice + D5 Empowerment: two OR suites allow scheduling flexibility and prevent bottlenecking. Each prep room is private and patient-controlled. No shared pre-op waiting in a corridor.
S3 Built
Private individual recovery bays, not open ward
D1 Safety + D9 Comfort: recovery happens in an enclosed, private bay rather than a curtained open ward. Patients cannot hear or be heard by others during the most physically vulnerable moment of their visit.
S3 Built
Staff garden and lounge directly off surgical corridor
D11 Play + D10 Movement: the staff lounge is positioned so surgical teams can step out without leaving the secure floor. Restoration is built into the spatial sequence, not located in a separate building or distant floor.
S1 Policy + S3 Built
- Standard exam tables, institutional overhead lighting
- No gown options or patient privacy protocol
- 1978 acoustic standards wall transmission likely
- Provider controls all sequencing patient waits passively
The problem: exam rooms are the highest-stakes spaces in this building. Re-traumatization risk peaks here, especially for patients with histories of medical gatekeeping, body-shaming, or non-consensual examination.

Gown options full wrap, top-only, shorts patient selects before provider enters
D6 Choice + D5 Empowerment returning bodily autonomy to patients at the moment of maximum physical vulnerability.
S1 Policy: a gown options protocol must be established as a clinical practice standard, staff must be trained not to override patient selections, and options must be maintained as part of room preparation procedure. · S3 Built: met through procurement of multiple gown types and storage within the exam room, a spatial and material design decision.
Patient-controlled dimmer + signal light outside door patient indicates readiness
D5 Empowerment + D2 Trustworthiness the provider does not enter until the patient signals. This reversal of control is clinical, not aesthetic.
S1 Policy: the provider entry protocol, waiting for patient signal before entering, is a clinical practice policy that staff must be trained to follow consistently; the technology is inert without the behavioral commitment. · S3 Built: met through electrical installation of dimmer controls and door signal light, a built environment specification.
Mirror on swivel mount patient can face it away at any time
D6 Choice + D9 Comfort body image dysphoria can be acute in clinical settings; the mirror is present but not mandatory.
S3 Built: met through fixture specification, a swivel-mounted mirror is a hardware decision with direct impact on patient agency over their visual environment.
"What to Expect" laminated card for each procedure type
D2 Trustworthiness + D1 Safety prepared patients experience measurably less re-traumatization; the unknown is its own trigger.
S1 Policy: creating, reviewing, and updating procedure-specific patient education materials is a clinical communications policy, content must be approved by providers and kept current with practice changes. · S2 Process: directly informed by lived experience, knowing what the surgeon was going to do before it happened, and what recovery would feel like, was a gap identified through the design process that shaped this intervention.
Patient community photography wall diverse representation of bodies and identities
D7 Equity + D9 Comfort patients see their own diversity reflected in the space before a clinical interaction begins.
S2 Process: participatory selection of images, centering trans, nonbinary, and BIPOC bodies chosen in consultation with community members, is a design process method that prevents the wall from reproducing the same narrow representation it is meant to counter. · S3 Built: met through physical installation, photography scale, framing, layout, and lighting within the exam room are spatial design decisions.
Side-by-side seating at a shared desk or table, provider and patient review the care plan as partners
D4 Collaboration + D2 Trustworthiness: the exam room layout physically enacts the clinical relationship. Across-the-desk seating positions the provider as authority and the patient as subject. Side-by-side seating at a shared surface positions them as co-authors of the care plan. For trans patients who have spent years navigating gatekeeping, this shift in spatial grammar is legible and meaningful.
S1 Policy: providers must be trained to use the collaborative seating, a desk layout means nothing if the provider defaults to standing over the patient. · S2 Process: shared decision-making frameworks (asking patients to name their goals before the provider names a plan) are a clinical process design, not just furniture. · S3 Built: met through furniture specification, a shared desk or table in place of the standard provider desk is a room layout decision.

Surgical Suite, Building B. Biophilic mural wall on wipeable high-pressure laminate, sage green modular panels, integrated acoustic ceiling grid with perimeter LED strip, articulating surgical light arm, and solid-core flush door. All surfaces sanitation-compliant. Domains: Safety (D1), Trustworthiness (D2), Empowerment (D5), Choice (D6), Equity (D7), Comfort (D9).

An emerging precedent: some contemporary surgical suite designs now incorporate frosted or translucent glazing, introducing diffused daylight without compromising patient privacy or sterile field integrity.
Emerging Practice · Windows in Surgery
More and more designers are now finding ways to bring diffused natural light into surgical spaces. While maintaining sterile conditions and full privacy, frosted glazing can reduce the environmental anxiety of the operating room without compromising clinical function.
Biophilic forest mural on wipeable high-pressure laminate wall panel
D9 Comfort + D7 Equity: the last thing a patient sees before anesthesia is a sunlit Pacific Northwest forest, not an institutional ceiling. Nature imagery measurably reduces pre-operative anxiety. HPL surface is fully cleanable to OR sanitation standards.
S3 Built: met through material specification, high-pressure laminate with printed mural finish is a surface upgrade, not a structural change, and is compatible with standard OR disinfection protocols.
Sage green modular wall panels, sanitation-compliant, eye fatigue–reducing color
D9 Comfort + D6 Choice: green is clinically documented to minimize eye fatigue during long procedures for surgical teams, while creating a warmer visual environment for the patient. Modular panels are seamless, nonporous, and fully wipeable.
S3 Built: wall panel color and material are a specification decision, no structural change required, and the modular system allows future reconfiguration.
Patient-ready signal panel, patient signals readiness before surgical team enters
D5 Empowerment + D2 Trustworthiness: even at the moment of maximum vulnerability, the patient retains one act of agency, signaling when they are ready. Providers do not enter until the light activates. This reversal of control is clinical, not cosmetic.
S1 Policy: the entry protocol, providers wait for patient signal, must be a surgical team behavioral standard, trained and enforced. The panel is inert without the cultural commitment behind it. · S3 Built: met through electrical installation of a wall-mounted signal panel, a low-cost built environment addition.
Solid-core flush door with acoustic perimeter seal, no window, full privacy
D1 Safety + D2 Trustworthiness: a windowless solid-core door means conversations inside the OR are not visible or audible from the corridor. For trans patients whose prior experiences include exposure, this baseline privacy is non-negotiable.
S3 Built: met through door specification, solid-core construction with acoustic frame seal is a hardware upgrade within the existing rough opening, no structural work required.
Surgical gown + patient-sized scrubs option stocked at patient hook near entry
D6 Choice + D5 Empowerment: patient-sized scrubs as an alternative to standard gowns, visible, pre-selected by the patient, hung and waiting when they enter. Bodily autonomy extends into the OR itself.
S1 Policy: procurement and stocking of patient-sized scrubs, and a protocol for patients to select their garment type in pre-op, is a supply chain and clinical practice policy. The hook on the wall means nothing without the options behind it.
Patient chooses the song they fall asleep to under anesthesia
D6 Choice + D5 Empowerment + D9 Comfort: at the moment of maximum vulnerability, when a patient surrenders bodily control to a surgical team, offering one small act of agency matters. Pre-op intake asks: is there a song you want playing as you go under? The clinical team plays it. The surgery does not change. The felt experience does.
S1 Policy: this is a zero-cost policy intervention. It requires a single intake question, a speaker in the OR, and a surgical culture that treats the answer as worth honoring. No structural change. No additional equipment. Just a decision to ask.
Patient-led pre-op check-in: patient confirms pronouns, names concerns, affirms consent in their own words before the team begins
D4 Collaboration + D5 Empowerment: the standard pre-op flow positions the surgical team as the initiating authority. Reversing this, the patient speaks first, names what they need, and the team listens before beginning, reframes the moment of maximum vulnerability as one of shared preparation rather than institutional procedure. This is not a formality. For patients with histories of medical trauma, being heard before the procedure matters as much as the procedure itself.
S1 Policy: the patient-led check-in must be a written surgical protocol, trained across the full team including anesthesiology and nursing, not left to individual provider discretion. · S2 Process: the check-in is a clinical process design decision, a structured moment of co-authorship built into the surgical sequence before sterile field is established.

Mental Health Therapy Room, Building B, Second Floor. Equal-height seating, terracotta boucle patient chair with throw blanket, sage accent wall, fabric acoustic panels, frosted lower window, floor lamp, living plant. No desk. No clock. No clinical equipment.
Equal-height, equal-weight seating, no therapist desk, no power differential in furniture
D7 Equity + D9 Comfort: two chairs of equivalent height and visual weight, angled, not face-to-face, refuse the hierarchy built into desk-and-chair or elevated-provider layouts common in clinical settings. The physical arrangement of a therapy room encodes a power relationship.
S3 Built: met through furniture selection and spatial arrangement, chair height, weight, material, and angle relative to each other are interior design decisions with direct clinical implications for how power is experienced in the room.
Throw blanket on patient chair + floor cushion nearby, choice without asking
D6 Choice + D5 Empowerment: comfort objects and positional options are present without requiring the patient to request them. Asking to be comfortable is its own barrier, these objects are simply there, patient-accessible at any moment without negotiating for them.
S3 Built: met through procurement and placement, the throw and cushion are design elements, not afterthoughts. Their position communicates that patient comfort is anticipated, not accommodated.
Sound machine at door + fabric acoustic panels, acoustic privacy visible and felt
D1 Safety + D2 Trustworthiness: trans patients have been outed in clinical settings by being overheard. The sound machine is deliberately visible, it signals the room was designed for confidentiality. Fabric acoustic panels absorb sound while reading as texture and warmth rather than clinical infrastructure.
S3 Built: met through technology installation and material specification, sound machine placement, panel dimensions, fabric density, and mounting location are acoustic and design decisions working in concert.
No clock, no desk, no documentation apparatus visible during session
D2 Trustworthiness + D5 Empowerment: a visible clock positions the patient as performing within an allocated time. A desk and screen between clinician and patient creates a documentation apparatus that competes for clinician attention. Removing both signals this hour belongs to the patient.
S1 Policy: when and how documentation happens is a clinical workflow policy decision determining whether the patient experiences full clinician presence. · S3 Built: met through room programming, the absence of desk and clock is a design decision about what is not installed.
Frosted lower window + linen shade, natural light without visual exposure
D6 Choice + D1 Safety: natural light supports emotional regulation; visual exposure undermines it. Frosted glazing on the lower half admits warm diffused light while preventing sightlines in, the patient can be seen neither from corridor nor exterior.
S3 Built: met through glazing specification and window treatment, frost height and shade mounting are material decisions that resolve the conflict between daylight and privacy.

Physical Therapy & Post-Op Rehabilitation, Building B, Second Floor. Wood slat accent wall, patient pacing panel, privacy curtain, angled mirror, modern parallel bars, mat zone, warm pendant lighting, living plants.
Patient pacing panel: "READY / NEED A MOMENT", patient initiates each session
D5 Empowerment + D2 Trustworthiness: post-surgical bodies are not on the clinician's timeline. The patient signals readiness before touch or movement begins, a structural reversal of the default clinical power dynamic critical in a space involving physical contact.
S1 Policy: clinicians waiting for patient signal must be a written PT practice standard, the panel is inert without behavioral commitment. · S3 Built: met through installation of a two-button wall panel near room entry.
Privacy curtain on ceiling track, open by default, patient-controlled
D6 Choice + D1 Safety: for trans patients with histories of non-consensual examination, control over physical exposure during PT is a safety matter. The curtain open by default signals option rather than routine exposure.
S3 Built: ceiling track mounted so curtain rests open by default, the default position is itself a design decision about what the space assumes.
Angled mirror, available for alignment feedback, not centered, not mandatory
D6 Choice + D5 Empowerment: body image dysphoria does not pause for rehabilitation. Mirror positioned so patients can orient away without disrupting the session, agency over the visual encounter with one's own post-surgical body.
S3 Built: mirror placement and mounting angle determine whether reflective feedback is offered or imposed, a hardware and layout decision.
Modern parallel bars + accessible mat zone, non-institutional aesthetic, all bodies served
D7 Equity + D9 Comfort: rehabilitation equipment specified without institutional signaling, clean-lined parallel bars and a flush mat surface serve a full range of mobility needs without broadcasting clinical limitation as deficit.
S3 Built: bar height, finish, and spatial relationship to the mat zone are specification decisions that determine whether adaptive equipment reads as dignified or medical.
Wood slat accent wall, warm pendant lighting, full-height window, living plants
D9 Comfort + D11 Play: biophilic and warm material design signals that movement is restorative, not punitive, countering clinical austerity that makes rehabilitation feel like obligation rather than care.
S3 Built: wood slat wall, glazing, pendant fixtures, and plant procurement are interior specification decisions requiring no structural change to the floor plate.

Irregular seating circle, no designated head
No seat encodes authority. The arrangement refuses hierarchy before a word is spoken.
Spatial equality is equity enacted, when every position carries equal status, group members arrive as peers, not as patients arranged around a provider.
S3 Built Environment
Mixed seating types + open wheelchair space in circle
Comfort chosen, not assigned. Wheelchair space is part of the circle, belonging, not accommodation.
Offering chairs, a floor cushion, a bench, and a loveseat means each person selects the body posture that feels safest. The wheelchair position is flush with the circle, not a gap or afterthought.
S3 Built Environment
Loveseat option
Someone can bring a support person, or simply spread out. The seat signals that connection is welcome.
Peer support is sometimes a body in the room, not a formal co-therapist, just someone who makes showing up possible. The loveseat holds that reality without singling anyone out.
S3 Built Environment
Water station + blankets, available without asking
Self-regulation without permission. Access is unconditional.
Requiring a person to ask for water or a blanket reintroduces a permission structure in a space meant to undo it. Ambient availability removes the ask entirely.
S3 Built Environment
Sound machine visible before entry
Confidentiality signaled before the door opens, not assumed, not invisible.
Placing the sound machine in view of the hallway communicates to anyone passing that what happens inside stays inside. Trust is built through legible, observable commitments.
S3 Built Environment
No clock, no whiteboard
The hour belongs to the group, not the agenda. Time is held by the facilitator, not posted.
A visible clock shifts attention toward ending. A whiteboard implies a lesson plan. Removing both returns authority over the session's shape to the group itself, a policy decision made legible through design.
S1 Policy & Practice → S3 Built Environment
Acoustic panels as textile art
Privacy infrastructure that does not announce itself. Safety built into the aesthetic.
When acoustic treatment doubles as artwork, woven panels, soft textiles, botanical prints, confidentiality becomes part of the room's warmth rather than a clinical signal. The space absorbs sound and holds people at once.
S3 Built Environment
Patient community photography wall
Trans and nonbinary bodies, chosen by community members, displayed at eye level before disrobing begins.
Seeing yourself in the room before the exam starts is a form of trustworthiness. The wall says: others like you have been here and were held. Participatory image selection (S2) grounds the S3 installation in authentic representation.
S3 Built Environment
Lounge chair alongside exam table
Patients can receive results, ask questions, or simply wait in soft seating rather than on the table.
The exam table is the most exposed position in a clinical room. Offering a chair before and after clinical contact restores the patient to a position of equal footing, literally and socially, for the parts of the visit that do not require the table.
S3 Built Environment
Warm wood tones, plants, natural light
Material and biophilic palette signals care rather than procedure. The room does not announce itself as clinical before the patient is ready.
For patients returning every three months over years, the room accumulates meaning. A room that feels warm and living reduces anticipatory cortisol and supports the kind of honest conversation that endocrinology depends on.
S3 Built Environment
Provider entry signal panel
Patient signals readiness before the provider enters. The door does not open until the patient initiates.
At maximum vulnerability, the patient retains one act of agency. For trans patients with histories of clinical violation, the ability to control the moment of exposure is not a courtesy; it is a clinical safety condition. The S1 protocol is enforced through the S3 panel.
S1 Policy & Practice, S3 Built Environment
Gown and drape options pre-selected by patient
Multiple options hung and visible on arrival. Patient chooses coverage before the provider enters.
For endocrinology and hormone care specifically, repeated physical exposure over years of treatment means gown choice accumulates into a pattern of self-knowledge. Visible options eliminate the need to ask.
S3 Built Environment